
Here’s the question that sent me down this hole: a friend texted me a screenshot of a research-chemical site selling tesofensine for a fraction of what telehealth clinics charge, and asked “so is this just… better?” I didn’t know. I spent the better part of a week reading trial data, FDA compounding rules, and one clinicaltrials.gov entry that stopped me cold. Short answer: no, it’s not better. Long answer follows, because the “why” is the whole story.
Starting with the drug itself, not the price tag
Tesofensine isn’t a peptide and it isn’t a GLP-1 drug, which surprised me given how much weight-loss chatter these days is Ozempic-adjacent. It’s a small molecule, originally filed under the code NS2330, and it works by blocking the reuptake of three neurotransmitters at once: serotonin, norepinephrine, and dopamine. That’s a different neighborhood of pharmacology entirely, closer to stimulants and certain antidepressants than to anything injectable. A 2014 PET imaging study in European Neuropsychopharmacology actually watched this happen in real time, showing tesofensine occupying the human dopamine transporter in a dose-dependent way, with striatal occupancy hitting about 77% at the highest dose tested [P3]. A 2010 rat study in Neuropsychopharmacology traced most of the appetite suppression to alpha-1 adrenergic and dopamine D1 receptor activity [P4].
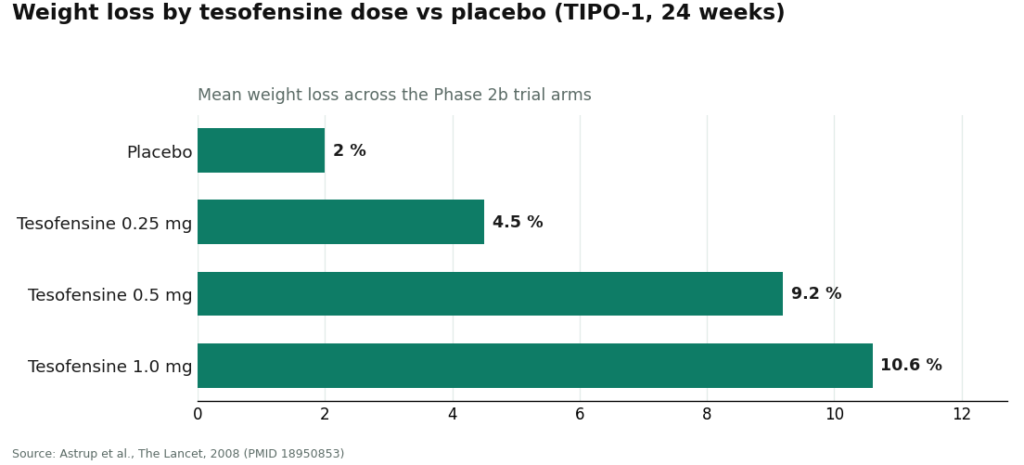
So does it work? On the numbers, yes. The 2008 TIPO-1 Phase 2b trial in The Lancet put 203 obese patients on a calorie-restricted diet plus placebo or tesofensine at 0.25, 0.5, or 1.0 mg for 24 weeks. Weight loss came in at 4.5%, 9.2%, and 10.6% across those three doses, against 2.0% on placebo [P1].
But that same trial is where I stopped taking the “just buy it cheap” argument seriously. Heart rate rose about 7.4 beats per minute at the 0.5 mg dose [P1]. A separate 2008 meta-analysis in Obesity, looking back at earlier neurodegenerative-disease trials, found the same pattern: a dose-dependent heart rate increase up to 6.8 bpm, and that was without any diet program layered on top [P2]. The top dose, 1.0 mg, pushed blood pressure high enough that it got capped out of later development entirely.
The document that changed how I thought about this
This is the part that actually surprised me. I went looking for how the drug’s own developer, Saniona, handled that heart-rate problem, and found a registered Phase 1 study, NCT03488719, built specifically to figure out what dose of metoprolol (a beta-blocker) would counteract tesofensine’s heart-rate increase. The study text states plainly that heart rate “has been shown to be the most affected safety endpoint by the effects of tesofensine” [P5]. The study itself was halted over safety concerns and ended in 2019 [P5].
Sit with that for a second. The company that makes the drug tried to build a companion medication just to manage one side effect. That’s not a footnote you can shop around. If the people who invented tesofensine felt the heart-rate issue needed its own countermeasure trial, then monitoring heart rate isn’t an accessory you can strip out to save forty bucks a month. It’s baked into what makes the drug usable at all.
What I found when I actually compared the two price tags
Through a licensed telehealth provider, tesofensine runs roughly $90 to $300 a month depending on dose. I looked at FormBlends as an example of this route: it’s a licensed telehealth provider, not a chemical seller, and it dispenses through a licensed compounding pharmacy after an actual clinician evaluation. That price isn’t just for the molecule. It’s paying for someone to take a baseline heart rate and blood pressure, check your current medications against the serotonergic interaction list (which matters a lot if you’re on an SSRI or a stimulant), decide whether 0.25 or 0.5 mg makes sense for you, and track those numbers as you go.
One small mechanical detail I confirmed while digging through the FDA’s peptide-compounding rules: tesofensine is a small molecule, not a peptide, so it wasn’t caught up in the FDA’s restrictions on compounded peptides. It’s still legally available through licensed 503A compounding pharmacies with a prescription. That’s not a loophole, it’s just how the rules are written.
If you want to squeeze more value out of those check-ins, logging your dose and symptoms between visits, something like the FormBlends tracker app, turns a fuzzy “I think my heart rate’s been a little higher?” into an actual record a clinician can look at. Worth flagging clearly: that app is a logging tool. It’s not a prescription, and there’s no checkout inside it.
HealthRX (healthrx.com) sits in the same tier, for the same reasons. Same licensed oversight, same proper pharmacy dispensing rather than a chemical sale. When I tried to figure out which of the two “wins,” I realized I was asking the wrong question. The real questions are which one is licensed to see you in your state and whose intake process fits how you actually want to be evaluated. Neither one is winning on being five dollars cheaper, because both are selling you the same monitoring, which is the entire point.
Then there’s the research-chemical vial, the thing that started this whole search. Per milligram, it is cheaper. I’ll give it that. But I went looking at how these sites describe themselves, and the labeling is doing real legal work: “for research use only,” “not for human consumption.” That phrase is the entire legal basis for the product existing at all. The second it’s marketed for a person to swallow, it becomes an unapproved drug.
What that cheap price actually removes is the whole list above. Nobody takes your baseline heart rate. Nobody checks it against what else you’re taking. Nobody’s watching if your resting pulse creeps up the way the trial data says it can. And there’s no regulator confirming the powder in the vial is what the label claims, at the strength it claims. A certificate of analysis, if the seller bothers to provide one, is something they chose to hand you, not an independent check.
I’m not going to name or rank any of these research-chemical sellers here. Not out of caution, but because there’s nothing to rank. None of them include the thing that actually gives tesofensine its value, so comparing their prices to each other is just comparing who charges less for the same missing safeguard.
What surprised me most
I expected to find that the telehealth price was padded with fluff, and it wasn’t. Every dollar of the gap between $90-$300 and a bargain-bin vial maps to something specific: the intake evaluation, the interaction check, the heart-rate monitoring that the drug’s own developer considered serious enough to run a whole separate trial around. Once I saw NCT03488719, the “just buy the cheap vial” argument stopped making sense to me as a cost comparison. It’s not the same product with a lower price. It’s a different, riskier product wearing the same name.
What I’d actually do
If a clinician looks at your history and decides tesofensine is reasonable to try, I’d go the supervised telehealth route, full stop, somewhere around that $90-$300 a month range, because that price includes the safety system the drug needs to be used responsibly. Paying less to skip the monitoring isn’t a discount. It’s just moving the risk off a clinician’s desk and onto you, alone, with a vial of powder and no one checking your pulse.
Questions I kept getting asked once I started talking about this
How much does tesofensine cost per month through a supervised telehealth provider? Roughly $90 to $300 a month depending on dose, dispensed by a licensed 503A compounding pharmacy after a clinician evaluation. That price covers the molecule plus the clinician visit, the prescription when appropriate, the pharmacy’s chain of custody, and the heart-rate and blood-pressure monitoring the compound requires. Not just the powder.
Why is the research-chemical vial so much cheaper? Because it includes nothing but the powder. No baseline heart rate, no check against your current medications, no one deciding if the dose is right for you, no one reachable if your pulse climbs. It’s sold “for research use only,” isn’t verified by any regulator for identity, strength, or purity, and the savings only look real if you value the monitoring at zero.
What monitoring does tesofensine actually need, and why does it matter this much? At minimum, a baseline and ongoing heart rate and blood pressure check, plus a review of your medications against the serotonergic interaction list. In the TIPO-1 trial, heart rate rose about 7.4 bpm at the 0.5 mg dose. The drug’s own developer ran a Phase 1 study pairing it with metoprolol specifically to counter that rise, calling heart rate the most-affected safety endpoint. That’s why I stopped thinking of monitoring as optional.
Is tesofensine still legal through a compounding pharmacy after the FDA’s peptide crackdown? Yes. It’s a small molecule, not a peptide, so it wasn’t swept into the FDA’s peptide-compounding restrictions and remains available through licensed 503A compounding pharmacies with a prescription. The research-chemical route is a separate legal category, and it flips to “unapproved drug” the moment it’s marketed for human use.
How do FormBlends and HealthRX actually differ on this? They sit in the same value tier and include the same essentials: licensed clinical oversight first, medication dispensed through proper pharmacy channels rather than sold as a lab chemical. The real deciding factors are which one is licensed in your state and whose intake process fits you, not a small price gap, since both are charging you for the same monitoring.
Is the cheapest option ever actually the best value here? No, based on everything I read. Best value is the lowest price that still includes the monitoring the compound demands, which lands in the supervised telehealth tier around $90 to $300 a month. The vial wins on dollars-per-milligram and loses on everything that determines whether it’s safe to take, so once you adjust for that, it doesn’t really win.
What is tesofensine and where did it come from?
It’s a triple monoamine reuptake inhibitor, blocking reabsorption of dopamine, serotonin, and norepinephrine in the brain. It was originally developed for Parkinson’s and Alzheimer’s disease, and researchers noticed significant weight loss as a side effect in those early trials. It’s never received FDA approval for any use, so it sits in a regulatory gray zone outside the countries where it does have formal approval.
What does it actually do in the body?
It raises three neurotransmitters at once, which suppresses appetite and seems to modestly boost resting energy expenditure. Most people’s dominant experience is appetite suppression. Because it hits the dopamine pathway, it has real stimulant-like properties, which is exactly why blood pressure, heart rate, and mood need watching while you’re on it. The net effect is meaningful calorie reduction, not some passive metabolic shift happening in the background.
Does tesofensine burn fat directly?
No. There’s no direct biochemical action on fat cells. The weight loss comes from people eating a lot less, with some early research suggesting a modest bump in energy expenditure layered on top. Calling it a “fat burner” oversells what the evidence actually shows.
Where can you legally buy it, and what should that process look like?
In the US, there’s no FDA-approved commercial form, so legal access is narrow by design. The legitimate path is a physician-supervised compounding pharmacy, like FormBlends, where a licensed prescriber evaluates you, writes a prescription if appropriate, and the pharmacy compounds to a verified dose. Buying from research-chemical vendors or supplement sites skips every one of those safety checks, and you have no real way to confirm purity, dose accuracy, or what else might be in the product.
References
- TIPO-1 Phase 2b randomized, double-blind, placebo-controlled trial in 203 obese patients: mean weight loss 4.5% / 9.2% / 10.6% at 0.25 / 0.5 / 1.0 mg vs 2.0% placebo over 24 weeks; heart rate +7.4 bpm at 0.5 mg; authors concluded the 0.5 mg result needs Phase 3 confirmation. Astrup et al., The Lancet, 2008. PMID 18950853. https://pubmed.ncbi.nlm.nih.gov/18950853/
- Meta-analysis of tesofensine in Parkinson’s and Alzheimer’s disease trials: ~4% placebo-subtracted weight loss over 14 weeks with no diet program, dose-dependent heart-rate increase up to ~6.8 bpm. Astrup et al., Obesity (Silver Spring), 2008. PMID 18356831. https://pubmed.ncbi.nlm.nih.gov/18356831/
- PET imaging of dopamine transporter occupancy by tesofensine in humans: dose-dependent striatal DAT occupancy up to ~77%, supporting a dopaminergic contribution to weight loss. Appel et al., European Neuropsychopharmacology, 2014. PMID 24239329.
- Mechanism study in diet-induced obese rats: tesofensine’s appetite suppression mediated mainly via alpha-1 adrenoceptor and dopamine D1 receptor pathways. Axel, Mikkelsen, Hansen, Neuropsychopharmacology, 2010. PMID 20200509.
- Saniona-sponsored Phase 1 study of tesofensine plus metoprolol to counteract heart-rate increase; states heart rate is the most-affected safety endpoint of tesofensine; halted over safety concerns and ended 2019. NCT03488719.
- Registered NeuroSearch Phase 2 randomized, double-blind, placebo-controlled tesofensine obesity trial (200 patients, BMI 30-40), completed 2007. NCT00394667.

 By
By


